Written for Erika Price’s Writing 150 class.
Many underestimate the magnitude of the global suicide problem. Self-destruction is the cause of 1.4% of all deaths worldwide—800,000 a year, or an average of one every forty seconds (“Preventing Suicide”). For smaller subgroups of the world’s population, this crisis is even more pressing: though it is the 15th leading cause of death overall, suicide is second only to accidents, motor vehicle and otherwise, for people aged 15 to 29 (“Preventing Suicide”). But these statistics still fail to capture the full scope of the problem; attempting suicide and failing is far more common than seeing it through, and having suicidal thoughts but never trying to carry them out is more common than either. According to data from the National Survey on Drug Use and Health, less than 4% of all suicide attempts in the U.S. in 2009 were successful—for every death by suicide, there were approximately twenty-five failed attempts (Crosby et al.). And yet the number of attempts is less than half of the number of people who made suicide plans, which in turn is less than a third of the number of people who reported having suicidal thoughts (Crosby et al.). Given this information, it sadly comes as no surprise that over half of American adults know someone who has taken his or her own life (“More than Half”).
Changes in policy and concerted efforts by large organizations—for instance, securing common jump sites or banning the importation of toxic pesticides—often have a beneficial effect on the suicide rate of the areas they influence (Hemmer et al., Gunnell et al.). However, most people have no say in how these programs are created or operated, so it is common for individuals to feel insignificant in comparison; it is easy to be overwhelmed by the prevalence and shock of suicide, believing ourselves powerless to stop it. This is dangerously untrue. At least equal in power to population-wide actions are the personal interactions between individuals. The same principles that drive large policies and programs are also applicable to how we think about and interact with people we are close to. By being aware of the risk factors for suicide and proactively seeking to help friends and family who may be struggling with suicidal thoughts, it is possible to prevent those thoughts from ever coming into fruition.
Friends
There is a wealth of evidence that social factors, such as friendship and social belonging, often play a role in the decision to commit suicide. One of the largest studies of its kind measured the associations between various self-reported friendship data, suicidal ideation, and suicidal behaviors in adolescents, and found that suicidal thoughts in youth are strongly affected by their social position amongst their peers (Bearman and Moody). Girls who do not belong to a tight-knit friend group or are otherwise socially isolated are far more susceptible to suicidal thoughts than those with cohesive friend groups; boys who attend schools that lack unity are far more likely to attempt suicide than boys in schools in which the social network is highly interwoven (Bearman and Moody). Additionally, the importance of strong social relationships does not diminish with age, although what constitutes a healthy relationship does change slightly; in the elderly, feeling lonely and lacking social support are among the most predictive measures of suicidal ideation (Chang et al.). Though the studies asked different questions of their participants, the underlying emotions—a need to belong, to be wanted, to have close relationships—are the same. Based on this knowledge, striving to include and befriend others is a logical preventative measure; it is an effective action that people of any age can take to decrease the likelihood of others experiencing suicidal thoughts.
But merely having strong and stable social connections is not enough; the behavior of one’s friends and other peers has an effect as well. Investigating the link between the type of friendships students have and their well-being and activity reveals that, in general, students with friends report greater happiness and engage in fewer delinquent behaviors, such as drinking and using drugs, than those who do not have friends; however, having certain types of friends puts students at greater risk of delinquency than having no friends (Güroğlu et al.). It depends on the person’s position within his social group; if he is perceived as a bully—aggressive and confident—or is withdrawn and often victimized, he is just as likely to participate in harmful, delinquent activities as those without friends (Güroğlu et al.). This is important to suicide research because delinquent behaviors like the ones above are strongly associated with suicidal thoughts, attempts, and completions (Thompson et al.).
Another study confirms and builds upon these claims with specific focus on ethnic differences; for European Americans, having delinquent friends is a risk factor for suicidal actions, while a more significant risk factor for Mexican Americans is having a discordant friend group (Winterrowd et al.). These findings suggest a universal need for social satisfaction and stability that is manifested differently as a result of differing expectations. Some people and cultures value interconnectedness more highly, some value their friends’ adherence to societal norms, and presumably other individuals and cultures value other measures of social success. Specific examples and studies are valuable as empirical evidence of the effects of social discontent, but they aren’t necessary for understanding how to prevent suicides. We intuitively understand what constitutes a harmonious friendship, so if we want to help people who are thinking about suicide or preemptively stop the thoughts from ever occurring, a worthwhile action we can take is to pay attention to those around us, recognize when they may be unhappy with their place in society, and respond by strengthening our relationships with them.
A Word on the Limitations of Statistics and Research
Interpersonal relationships can be divided broadly into two categories. The first is friendship and other social connections; the second is family. Thus far, I have discussed suicide in the context of the former category, but the latter merits a more detailed discussion, because the research is more extensive and our ability to affect outcomes in this sphere seems to be greater. Most research on this subject delineates specific actions and attitudes of family members that worsen suicidal intentions and others that improve them, and many publications conclude by claiming powerful, important results. The numerical and often black-and-white nature of statistics should not, however, lead you to believe that the causes of suicide are black and white. No individual is the average, and no two suicides have identical causes. Surviving family members are often consumed with guilt, believing they must have been able to do more. But there will always be inexplicable suicides, and there will always be lingering confusion following a tragic death. Do everything you can, but allow yourself to find peace if you have done your best; nothing is foolproof.
Family
The World Health Organization (WHO) mentions two major risk factors for suicidal thoughts and attempts in relation to the conduct of family: abuse and violence (“Preventing Suicide”). Many studies analyze the effects of adverse childhood experiences, and correlations have been found not just with suicide, but with nearly every imaginable negative health outcome later in life, including alcoholism, drug abuse, depression, smoking, sexually transmitted disease, obesity, heart disease, and even cancer (Felitti et al., van der Kolk et al.). Other research has found that suicide attempts in adults are most highly associated with childhood emotional abuse, though sexual and physical abuse are also extremely harmful (Dube et at., Dinwiddie et al., Fuller-Thomson et al., Liu et al.). The second factor mentioned by the WHO, violence, includes physical child abuse, but other actions are encompassed as well, such as wife battering. Domestic violence in all its forms has a lasting effect on children who experience or witness it, causing them to be up to three times more likely to attempt suicide in the future (Dube et al., Fuller-Thomson et al.). If suicidology allows us to draw any clear-cut, easy-to-implement, common-sense conclusions, this is one: do not abuse your children.
Romantic relationships, including marriage, are a major component of a person’s life satisfaction. However, the health and happiness benefits of being in a relationship are not unconditional; those in happy relationships report the lowest levels of suicidal ideation, but for those in unhappy or inharmonious relationships, risk factors for suicide are more common than for people who are single (Till et al. 12). A natural assumption is that conflict drives relationship unhappiness, and this is true with one caveat: the presence of conflict in a relationship has no adverse consequences on the couple’s happiness or health if the disagreements are resolved amicably. Every relationship inevitably has some conflict, but if the couple’s communication is healthy and their concerns are not left unresolved for long, then there are no discernable negative effects on occurrence of suicidal thoughts (Till et al. 13). This style of conflict resolution will also benefit their children, if they have any; quickly and respectfully resolving conflicts greatly decreases the likelihood of an abusive or violent home environment.
For married couples who have children, protecting them becomes a primary responsibility, largely because their ability to protect them is far greater than their ability to protect anyone else. One of the most basic and most potent ways to increase the safety of the home is similar to many large-scale suicide prevention efforts, such as the prohibition of pesticides and the securing of jump sites. These efforts focus not on mental health or individual help but on physically preventing people from killing themselves, despite their intentions to do so. This obvious counter-measure is supported by considerable research; many studies have found a higher incidence of adolescent suicide in homes containing a gun than in homes without (Brent et al. “Firearms”, Grossman et al.), and the same association exists for adults (Yeates et al.). It is well-known that many suicides are performed impulsively; a famous study on this subject published by the American Association of Suicidology found that for 36 out of 153 case subjects there was less than five minutes between the decision to commit suicide and the suicide itself (Simon et al. 52).
There is disagreement among researchers about the causes and implications of this and other similar findings, but at its simplest form they suggest that some suicides involve little forethought, so with easy access to a firearm, a suicidal urge that could have passed without incident may be fatal. The majority of suicides, however, are planned and forewarned, sometimes copiously (Smith et al.). Removing guns from the home is beneficial in these cases as well, because firearms are the most lethal method of suicide—2.5 times more likely to be fatal than the next most lethal method, suffocating—so forcing the victim to use a method other than a firearm decreases the likelihood that the attempt will be fatal (Shenassa et al.). Other safety measures, such as storing ammunition separately and keeping the weapon under lock and key, vary in their effectiveness, but none of them entirely mitigate the danger; having a gun in the house correlates with higher incidence of fatal suicides regardless of how it is stored (Brent et al. “The Presence”).
Another family decision that can have a positive effect on children is religious devotion and attendance of religious services. Numerous measures of religiosity, including personal commitment to faith, frequency of religious service attendance, finding comfort in religious beliefs, and associating often with people of the same faith, are associated with an attitude of greater disapproval toward suicide (Stack and Kposowa). In turn, people who believe suicide is not an acceptable resolution to personal problems are themselves less likely to commit suicide (Joe et al.). More specifically, there is evidence that the religious trait most efficacious in preventing suicide is orthodoxy, or strong belief in traditional religious values (Greening and Stoppelbein). This protection against suicide is plausibly caused by the motivational nature of beliefs pertaining to eternity, such as the threat of Hell and the promise of relief from suffering in Heaven. The community nature of churches and the support system they naturally provide are also likely factors.
However, the negative correlation between religiosity and suicidal ideation is not observed universally. For example, a study comparing college students in the American West and Beijing found opposite effects for the two ethnicities. Chinese students’ religiosity and suicidal ideation were positively correlated; that is, the more religious the student, the more likely he or she was to experience suicidal ideation (Zhang and Jin). These results show that although religious worship has benefits (such as optimism, a sense of belonging, and more harmonious family relationships) in many cultural settings, it is not inherently beneficial. When religion conflicts with those factors instead of improving them, as it seems to for Chinese college students, the effect reverses and suicidal ideation increases. This is seen most prominently not in Chinese universities, however, but in another subpopulation—a group so often misunderstood and mistreated that it must be addressed on its own.
LGBT Youth
LGBT youth are twice as likely to think about or attempt suicide as their heterosexual peers (Russell and Joyner). This trend is understood best in the context of Thomas Joiner’s Interpersonal Theory of Suicide, one of the most influential modern theories of suicide. Joiner asserts that two conditions must be met for someone to desire death— “thwarted belongingness and perceived burdensomeness”—and that every suicide is related fundamentally to these two psychological misalignments (Joiner 96). With this theory in mind, the suicide rate among LGBT youth is understandable. LGBT youth are persistently mistreated by their family and friends, made to feel abnormal, unnatural, and unwanted. A single statistic communicates the problem heartbreakingly well: 26% of LGBT youth are kicked out of their homes because of their sexual orientation (VanderWaal 73).
Even for those who are allowed to remain at home, being subject to endless skepticism, anger, confusion, and exasperation from parents and peers creates a feeling of isolation and of being a burden to others. This also explains why attendance of religious services has a detrimental effect on suicidal ideation of LGBT youth. Though some benefits, such as community support, remain, they are outweighed by familial rejection; religious parents are far more likely than nonreligious ones to respond negatively to children of nontraditional sexual orientation (Ryan et al. “Family Acceptance”). In fact, parents’ acceptance of their LGBT children is seemingly among the most influential factors I have discussed.
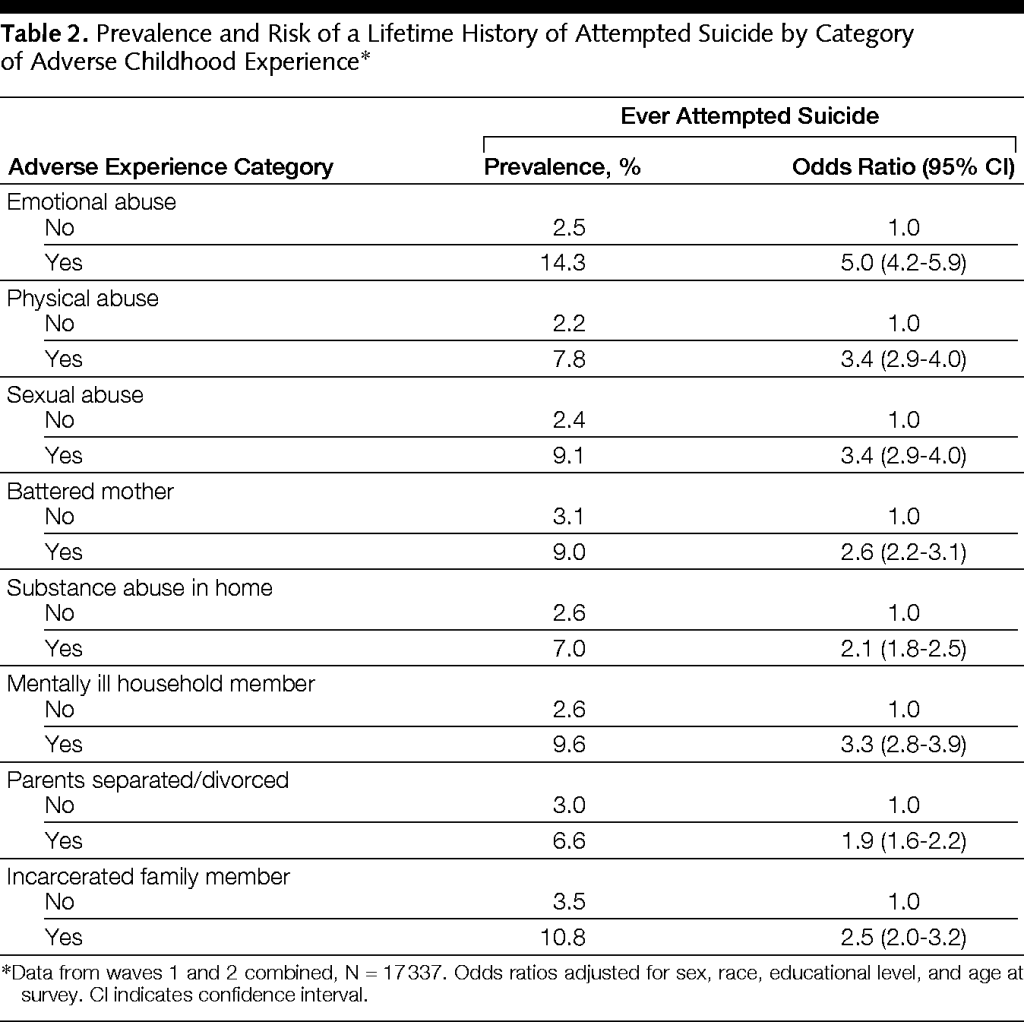
Data from LGBT young adults with differing family relationships show that those who report low levels of family acceptance are between 3 and 8.4 times more likely to have attempted suicide than those whose families were highly supportive (Ryan et al. “Family Acceptance”, Ryan et al. “Family Rejection”). To grasp the horrendous magnitude of those odds, consider this chart, which shows odds ratios for various harmful childhood experiences. Those who endured childhood sexual assault, for example, are between 2.9 and 4.0 times more likely to have ever attempted suicide than those who did not (Dube et al.). Think about that: for LGBT youth, feeling rejected by their families increases the odds of a future suicide attempt just as much as, and possibly even more than, being sexually assaulted.
Conclusion
At the conclusion of the discussion of suicide, it would be remiss to neglect to mention one final risk factor. Depression is by far the most common psychiatric disorder in suicide victims, the commonality linking many who are suffering and who have passed (Meyer). The American Association of Suicidology reports that more than half of suicide victims are depressed; depressed individuals’ risk of suicide is 25 times higher than the general population (“Facts”). The identification and treatment of depression is too vast a topic to address fully in this paper, but a summary of some research as it relates to the subject at hand is relevant.
In short, treating depression is effective, vastly more so than hoping it will go away on its own; medication, psychotherapy, and even lifestyle changes such as regular exercise have all been shown to lessen dejection and reduce suicide attempts (Craft and Landers, Simon and Savarino). If someone is clinically depressed, his or her risk of suicide should not be understated or ignored. Depression is an illness, not a choice, and not to treat it as such is dangerous.
Remember, above all, that suicide is preventable. Remember the risk factors, recognize when they are present, and have the courage to talk to friends or family members about whom you are concerned. Asking them about suicide will not push them over the edge or put the thought of suicide in their mind; all the evidence tells us that directly asking if someone is considering suicide lessens suicidal intent and can open the door to more help and treatment (Dazzi, Mathias). Suicide is a terrible epidemic, but it isn’t an unbeatable one: our actions can save lives.
Works Cited
Bearman, Peter S. and James Moody. “Suicide and Friendships Among American Adolescents.” American Journal of Public Health, Vol. 24, No. 1, American Public Health Association, 2004.
Brent, David A., et al. “Firearms and adolescent suicide. A community case-control study.” American Journal of Diseases of Children, Vol. 147, No. 10, pp. 1066-1071, Oct. 1993.
Brent, David A., et al. “The Presence and Accessibility of Firearms in the Homes of Adolescent Suicides.” Journal of the American Medical Association, Vol. 266, No. 21, pp. 2989- 2995, American Medical Association, 1991.
Chang, Qingsong, et al. “A meta-analytic review on social relationships and suicidal ideation among older adults.” Social Science and Medicine, Vol. 191, pp. 65-76, Elsevier, Oct. 2004.
Craft, Lynette L. and Daniel M. Landers. “The Effect of Exercise on Clinical Depression and Depression Resulting from Mental Illness: A Meta-Analysis.” Journal of Sport & Exercise Psychology, Vol. 20, No. 4, pp. 339-357, 2011.
Crosby, Alex E., et al. “Suicidal thoughts and behaviors among adults aged ≥18 years–United States, 2008-2009.” Centers for Disease Control and Prevention, 21 Oct. 2011.
Dazzi, T., et al. “Does asking about suicide and related behaviours induce suicidal ideation? What is the evidence?” Psychological Medicine, Vol. 44, No. 16, Cambridge University Press, pp. 3361-3363, December 2014.
Dinwiddie, Stephen, et al. “Early sexual abuse and lifetime psychopathology: a co-twin-control study.” Psychological Medicine, Vol. 30, No. 1, pp. 41-52, 2000.
Dube, Shanta R, et al. “Childhood Abuse, Household Dysfunction, and the Risk of Attempted Suicide Throughout the Life Span: Findings From the Adverse Childhood Experiences Study.” Journal of the American Medical Association, Vol. 286, No. 24, pp. 3089-3069, 2001.
“Facts and Statistics.” American Association of Suicidology, 2015.
Felitti, Vincent J., et al. “Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study.” American Journal of Preventative Medicine, Vol. 14, No. 4, pp. 245-258, May 1998.
Fuller-Thomson, Esme, et al. “The association between adverse childhood experiences (ACEs) and suicide attempts in a population-based study.” Child: Care, Health, and Development, Vol. 42, No. 5, pp. 725-734, 2016.
Greening, Leilani and Laura Stoppelbein. “Religiosity, Attributional Style, and Social Support as Psychosocial Buffers for African American and White Adolescents’ Perceived Risk for Suicide.” Suicide and Life-Threatening Behavior, Vol. 32, No. 4, pp. 404-417, American Association of Suicidology, 2002.
Grossman, David C., et al. “Gun storage practices and risk of youth suicide and unintentional firearm injuries.” Journal of the American Medical Association, Vol. 293, No. 6, pp. 707-714, American Medical Association, 2005.
Gunnell, David, et al. “The impact of pesticide regulations on suicide in Sri Lanka.” International Journal of Epidemiology, Vol. 36, No. 6, pp. 1235-1242, 27 Aug. 2007.
Güroğlu, Berna, et al. “Similarity and Complementarity of Behavioral Profiles of Friendship Types and Types of Friends: Friendships and Psychosocial Adjustment.” Journal of Research on Adolescence, Vol. 17, No. 2, pp. 357-386, Society for Research on Adolescence, May 2007.
Hemmer, Alexander, et al. “Comparing Different Suicide Prevention Measures at Bridges and Buildings: Lessons We Have Learned from a National Survey in Switzerland.” Social Science and Medicine, Vol. 70, No. 10, pp. 1626-1632, May 2010.
Joe, Sean, et al. “Suicide Acceptability is Related to Suicide Planning in U.S. Adolescents and Young Adults.” Suicide and Life-Threatening Behavior, Vol. 37, No. 2, pp. 165-178, American Association of Suicidology, Jul. 2009.
Joiner, Thomas E. Why People Die By Suicide. Harvard University Press, 2005. Liu, Jianbo, et al. “Associations between suicidal behavior and childhood abuse and neglect: A meta-analysis.” Journal of Affective Disorders, Vol. 220, pp. 147-155, 2017.
Mathias, Charles W., et al. “What’s the Harm in Asking About Suicidal Ideation?” Suicide and Life-Threatening Behavior, Vol. 42, No. 3, pp. 341-351, American Association of Suicidology, April 2012.
Meyer, Cheryl L., et al. Explaining Suicide. Elsevier, 2017.
“More Than Half of Americans Know Someone Who Committed Suicide.” Rasmussen Reports, 19 Sep. 2017.
“Preventing Suicide: A Global Imperative.” World Health Organization, 2014.
Russell, Stephen T. and Kara Joyner. “Adolescent Sexual Orientation and Suicide Risk: Evidence From a National Study.” American Journal of Public Health, vol. 91, no. 8, 2001, pp. 1276-1281.
Ryan, Caitlin, et al. “Family Acceptance in Adolescence and the Health of LGBT Young Adults.” Journal of Child and Adolescent Psychiatric Nursing, vol. 23, no. 4, 2010, pp. 205-213.
Ryan, Caitlin, et al. “Family Rejection as a Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young Adults.” Pediatrics, Vol. 123, No. 1, American Academy of Pediatrics, Jan. 2009.
Shenassa, Edmond, et al. “Lethality of firearms relative to other suicide methods: a population based study.” Journal of Epidemiology and Community Health, Vol. 57, No. 2, pp. 120- 124, BMJ Group, 2003.
Simon, Gregory E. and James Savarino. “Suicide Attempts Among Patients Starting Depression Treatment With Medications or Psychotherapy.” American Journal of Psychiatry, Vol. 164, No. 7, American Psychiatric Association, Jul. 2007.
Simon, Thomas R., et al. “Characteristics of Impulsive Suicide Attempts and Attempters.” Suicide and Life-Threatening Behavior, Vol. 32, No. s1, pp. 49-59, American Association of Suicidology, Dec. 2002. Smith, April R., et al. “Revisiting Impulsivity in Suicide.” Behavioral Sciences & the Law, Vol. 26, No. 6, pp. 779-797, John Wiley & Sons, 2008.
Stack, Steven and Augustine J. Kposowa. “Religion and Suicide Acceptability: A Cross National Analysis.” Journal for the Scientific Study of Religion, Vol. 50, No. 2, pp. 289- 306, Wiley-Blackwell, Jun. 2011.
Thompson, Martie P., et al. “Associations Between Delinquency and Suicidal Behaviors in a Nationally Representative Sample of Adolescents.” Suicide and Life-Threatening Behavior, Vol. 36, No. 1, pp. 57-64, American Association of Suicidology, Feb. 2006.
Till, Benedikt, et al. “Relationship Satisfaction and Risk Factors for Suicide.” Crisis: The Journal of Crisis Intervention and Suicide Prevention, Vol. 38, No. 1, pp. 7-16, Hogrefe, 2016.
VanderWaal, Curtis J., et al. “The Impact of Family Rejection or Acceptance among LGBT+ Millennials in the Seventh-day Adventist Church.” Social Work and Christianity, Vol. 44, No. 1 & 2, pp. 72-95, 2017.
van der Kolk, Bessel A., et al. “Childhood origins of self-destructive behavior.” American Journal of Psychiatry, Vol. 148, No. 12, pp. 1665-1671, Dec. 1991.
Winterrowd, Erin et al. “Friendship Factors and Suicidality: Common and Unique Patterns in Mexican- and European-American Youth.” Suicide and Life-Threatening Behavior, Vol. 41, No. 1, American Association of Suicidality, 2011.
Yeates, Conwell, et al. “Access to Firearms and Risk for Suicide in Middle-Aged and Older Adults.” American Journal of Geriatric Psychiatry, Vol. 10, No. 4, pp. 407-416, Elsevier, 2002.
Zhang, J. and Jin S. “Determinants of suicide ideation: a comparison of Chinese and American college students.” Journal of Adolescence, Vol. 31, No. 122, pp. 451-467, Elsevier, 1996.